
目次
現代の糖尿病・肥満症治療における食事療法は、かつての「一律のカロリー制限」や「厳しい糖質禁止」という我慢の時代を経て、全く新しいフェーズへと突入しています。
そのキーワードとなるのが、「緩やかな糖質制限(ロカボ)」、そして今話題の肥満・糖尿病治療薬の基盤でもある「インクレチンホルモン」です。
これら最新の医学概念を網羅し、日々の食卓で実行できる“最適解”として、なぜ今「地中海食」が最注目されているのかを解説します。
1. 食事療法のパラダイムシフト:カロリーから「質」へ
かつての食事指導といえば、「お米は1食○グラムまで」「1日○kcalに抑えてください」という、引き算の理論が中心でした。しかし近年の研究で、極端なカロリー制限や過度な糖質制限は、長続きしないばかりか、筋肉量を減らして逆に代謝を落とすリスクが指摘されています。
そこで登場したのが、「緩やかなロカボ(ローカーボ)」という概念です。 これは「糖質をゼロにする」のではなく、「1食あたりの糖質量を20〜40g(間食10g)程度に抑え、その分、タンパク質や良質な脂質はしっかり食べる」という、続けやすさを重視したアプローチです。食後の血糖スパイク(急上昇)を防ぐ上で、このロカボは非常に高い有効性が証明されています。
しかし、ここで新たな疑問が生まれます。 「糖質を減らした分、代わりに何をプラマイプラスで食べれば体(代謝)に一番良いのか?」
この問いに対する医学的な答えこそが、「地中海食」のブレンドなのです。
2. 鍵を握る「インクレチンホルモン」:腸から代謝を上げる
最新の肥満・糖尿病治療を語る上で外せないのが、「インクレチン(GLP-1など)」というホルモンです。これは私たちが食事をしたときに「腸」から分泌されるホルモンで、以下のような驚くべき働きを持っています。
-
膵臓に働きかけ、血糖値が高いときだけインスリンを適切に分泌させる
-
胃の動きを緩やかにし、 糖の吸収をインテリジェントに遅らせる
-
脳の満腹中枢に刺激を送り、自然な満腹感をもたらして食欲を抑える
現在、非常に高い効果を上げている最新の注射薬や内服薬(GLP-1受容体作動薬)は、このホルモンを人工的に体内で増やすものです。しかし実は、「日々の食事の選び方次第で、このインクレチンを自分の腸からたっぷりと分泌させられる」ことが分かってきました。
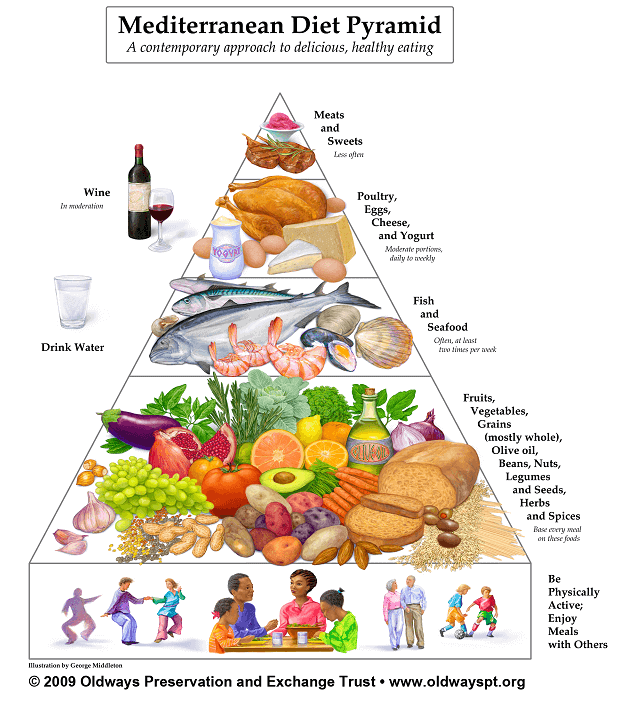
3. 最新栄養学の最適解:「ロカボ×インクレチン」を満たす地中海食
緩やかなロカボを満たしつつ、自前のインクレチンホルモンを最大限にドライブさせる——。この2つの条件をパーフェクトにクリアする食事が、まさに「地中海食」のパターンです。
地中海食がなぜ最適解なのか、その理由は腸と細胞のメカニズムにあります。
【地中海食が「最新の食事理論」に合致するメカニズム】
[地中海食の3大要素]
① 全粒穀物・豆類(豊富な水溶性食物繊維)
② エキストラバージンオリーブオイル(オレイン酸)
③ 青魚(EPA・DHA)
↓
[腸へのアプローチ]
• 食物繊維が腸内細菌によって「短鎖脂肪酸」に化ける
• 良質な脂質(オリーブオイル・魚油)が腸の細胞を直接刺激する
↓
[インクレチン(GLP-1)の自発的ドカンと分泌!]
↓
【結果】
• 緩やかなロカボとの相乗効果で、血糖スパイクが消失
• 膵β細胞の「過労死(小胞体ストレス)」を防ぎ、インスリン分泌能が蘇る
• 自然に満腹感が得られ、無理のない内臓脂肪減少へ
地中海食で推奨される大麦や玄米、大豆、根菜類には「水溶性食物繊維」が凝縮されています。これが腸の奥まで届くと、腸内細菌のエサとなり「短鎖脂肪酸」という物質に変わります。この短鎖脂肪酸と、オリーブオイルの主成分であるオレイン酸が、腸にあるL細胞をパチッと刺激し、内因性のGLP-1(インクレチン)を分泌させる強力なスイッチになるのです。
結論:お薬に頼り切る前に、食卓に「地中海」の知恵を
現代の肥満症・糖尿病治療において、優れた新薬が登場したことは素晴らしい進歩です。しかし、それらの薬剤も「適切な食事」という土台があって初めて100%の力を発揮します。
糖質をただ敵視して減らすのではなく、「未精製の質の良い糖質(大麦や玄米)を適量摂り、油をエキストラバージンオリーブオイルに変え、お肉を少し減らしてお魚や大豆製品を増やす」。
この地中海食のスタイルこそ、最新の代謝医学、ロカボ理論、そしてインクレチン科学が導き出した、私たちの体が最も喜ぶ「食事療法の終着駅」と言えるでしょう。
The Metabolic Shift: Why Science is Abandoning Calorie Counting for the Mediterranean Paradigm
For nearly half a century, the global paradigm for treating obesity and type 2 diabetes was defined by a single, punishing directive: eat less, suffer more. Clinical nutrition was treated like a ledger of simple arithmetic. Patients were instructed to treat their bodies like thermal furnaces, cutting calories and tracking macronutrients with mathematical rigidity.
Yet, as global rates of metabolic syndrome continued their relentless ascent, the limits of this balance-sheet approach became painfully clear. Rigid calorie restriction routinely collapsed under the weight of human physiology; extreme carbohydrate deprivation, while temporarily suppressing blood glucose, proved unsustainable and occasionally detrimental to long-term vascular health.
Today, metabolic medicine is undergoing a profound paradigm shift. We are moving away from the quantitative tyranny of the calorie and toward a qualitative understanding of cellular signaling. In this new era, defined by the rise of smart weight-loss therapeutics and a deeper grasp of gut endocrinology, the medical establishment has arrived at an unexpected consensus. The ultimate intersection of modern metabolic science, sustainable carbohydrate management, and hormonal optimization is not a new synthetic molecule or a radical starvation trend. It is the centuries-old traditional Mediterranean diet.
The Low-Carb Evolution: Beyond the Binary Trap
To understand why the Mediterranean model represents the therapeutic zenith of modern nutrition, one must first look at the evolution of “Lo-Carb” philosophy. The early iterations of carbohydrate restriction operated on a crude, binary premise: all carbohydrates are toxic; all fats and proteins are benign. While highly effective at flattening immediate postprandial glucose excursions—the dangerous blood sugar spikes that damage vascular walls—the long-term execution often faltered. Replacing carbohydrates with a heavy influx of saturated animal fats and processed meats triggered a secondary crisis: an increase in visceral adiposity, ectopic fat deposition in the liver, and a marked rise in atherogenic low-density lipoprotein (LDL) cholesterol.
The contemporary medical answer to this dilemma is “Smart Carb” or flexible low-carbohydrate therapy—colloquially termed “Locabo” in progressive clinical circles. The objective is no longer the elimination of carbohydrates, but the strict curation of their quality.
This is where the Mediterranean diet functions as a perfect clinical glove. It does not strip the patient of carbohydrates; instead, it replaces refined sugars and ultra-processed grains with intact, low-glycemic index (GI) complex carbohydrates: whole grains like barley and farro, legumes, and fibrous vegetables. By altering the architecture of the meal, the intrinsic water-soluble fibers delay gastric emptying and slow down intestinal glucose absorption. The result is a natural, predictable flattening of the glycemic curve without forcing the patient into chronic, stressful ketosis.
The Incretin Revolution: Awakening the Body’s Internal Pharmacy
The most explosive disruption in modern endocrinology has undoubtedly been the advent of GLP-1 receptor agonists—blockbuster pharmaceutical agents that have transformed the treatment of obesity and type 2 diabetes. These synthetic molecules mimic incretins, naturally occurring hormones secreted by the distal gut following nutrient ingestion. Incretins are the conductors of the metabolic orchestra: they signal the pancreas to secrete insulin in a glucose-dependent manner, suppress glucagon, slow gastric motility, and cross the blood-brain barrier to bind with receptors in the hypothalamus, elegantly turning off the neurological drive to overeat.
However, the pharmaceutical gold rush has overshadowed a fundamental physiological reality: the human gut possesses an extraordinary, latent capacity to manufacture its own endogenous incretins. And the most potent bio-chemical trigger to awaken this internal pharmacy is the specific nutrient matrix found in the Mediterranean diet.
[ THE BIO-CHEMICAL INCRETIN CASCADE ]
Dietary Intake: Intact Water-Soluble Fibers & Extra Virgin Olive Oil (EVOO)
│
▼
[ Upper Gastrointestinal Tract ]
Delayed Gastric Emptying / Slow Glucose Absorption
│
▼
[ Distal Ileum & Colon ]
Microbial Fermentation of Fibers into Short-Chain Fatty Acids
│
▼
[ L-Cells Activation ]
Dual Stimulation via SCFA Receptors & Oleic Acid G-Protein Receptors
│
▼
[ Endogenous GLP-1 & PYY Secretion Explodes ]
│
┌──────────────────────────┴──────────────────────────┐
▼ ▼
[ Central Nervous System ] [ Pancreas ]
Hypothalamic Satiety / Satiation Glucose-Dependent Insulin Release
When a patient consumes the whole grains, seeds, and legumes central to the Mediterranean diet, these complex structures escape early digestion and arrive intact in the large intestine. Here, the gut microbiota ferments these fibers into short-chain fatty acids (SCFAs), such as butyrate and propionate. Simultaneously, the abundant consumption of extra virgin olive oil delivers high concentrations of oleic acid, a monounsaturated fatty acid (MUFA).
Both SCFAs and oleic acid act as precise chemical keys, binding to specialized G-protein coupled receptors on the surface of enteroendocrine L-cells. This targeted binding triggers a robust, physiological surge of native GLP-1 and Peptide YY (PYY). By changing the quality of the fuel, we effectively replicate the therapeutic pathways of modern weight-loss medication through the grocery cart, restoring metabolic harmony from the inside out.
Preserving the Core: Alleviating Pancreatic Beta-Cell Burnout
For patients trapped in the cycle of insulin resistance and obesity, the underlying pathophysiological tragedy is the gradual, silent exhaustion of the pancreas. Chronic overnutrition forces pancreatic beta-cells into a state of permanent overdrive, pumping out massive volumes of insulin to overcome peripheral resistance. This relentless biosynthetic demand induces catastrophic endoplasmic reticulum (ER) stress and mitochondrial fatigue within the islets—a state known as glucolipotoxicity. Under this pressure, beta-cells do not merely die; they undergo “dedifferentiation,” losing their cellular identity and reverting to an immature, non-functional state.
【 Beta-Cell Protection Dynamics 】
Standard Western Diet (High Saturated Fat + Refined Carbs)
➔ Chronic Glucolipotoxicity ➔ Severe ER Stress ➔ Beta-Cell Dedifferentiation (Loss of Function)
Mediterranean Diet (High MUFA/PUFA + Polyphenols + Low GI)
➔ Alleviated Peripheral Demand ➔ Reduced ROS ➔ Beta-Cell Preservation & Functional Recovery
The Mediterranean diet addresses this core vulnerability by mounting a multi-front defense.
-
Lowering Peripheral Demand: By improving peripheral insulin sensitivity through the actions of MUFAs and marine omega-3 fatty acids (EPA/DHA), the diet dramatically lowers the baseline requirement for insulin. The pancreas is finally allowed to step off the treadmill.
-
Quenching Cellular Stress: The diet is saturated with highly bioavailable dietary antioxidants and polyphenols, such as oleuropein and hydroxytyrosol from olive oil. These compounds neutralize reactive oxygen species (ROS) and downregulate the systemic nuclear factor-kappa B (NF-κB) inflammatory pathway.
By quenching the inflammatory fires in adipose tissue and reducing the work demand on the pancreas, the Mediterranean diet actively shields the beta-cell from apoptosis and dedifferentiation. It transitions the pancreatic microenvironment from a state of toxic exhaustion to one of metabolic recovery.
The Clinical Ultimatum
As metabolic medicine enters a more sophisticated era, the medical community must move past the simplistic, unsustainable dichotomy of choosing between low-calorie starvation or high-fat, aggressive carbohydrate elimination.
The Mediterranean diet is not an compromise; it is an intelligent synthesis. It successfully captures the glycemic stabilization of a controlled carbohydrate (Lo-Carb) diet, utilizes the advanced endocrine pathways of modern incretin science, and delivers the profound cellular protection required to halt the progression of metabolic disease. For clinicians and patients navigating the complex waters of modern metabolic health, this ancient dietary pattern remains the definitive, scientifically validated destination.